|
|
Aticella, |
|
|
Aticella, |
1. Infertility-
Causes (Ford);
2.
Dign Person (2008) on treatments - no
1-5, 12-13;
3.
Naprotechnology;
4.
Debated Treatments - GIFT; 5.
Male
Infertility:,Phthalates, Estrogen, and Testosterone
1. FORD
on INFERTILITY:
Causes and Medical Treatments
The Prenatal Person:
Ch.
6:
INFERTILITY
and
ARTIFICIAL
REPRODUCTIVE
TECHNOLOGY
[6.1.1]
Incidence and causes
Ethical debates have not ceased on in vitro fertilization (IVF) since the birth of Louise Brown, the first IVF baby, was born on July 25, 1978 in the UK. In Australia in 1996 there were 3,164 births after artificial re-productive technology (ART), accounting for 1.2 percent of all births.[1] Before entering into a discussion and evaluation of the ethical issues arising from the treatment of infertility, it is necessary to understand what is meant by infertility, its treatment options, their success rates, and the burdens experienced by couples undergoing treatment.[2]
It is important to distinguish infertility from sterility. A person who is unable to generate any offspring is sterile, e.g. a woman who has no ovarian follicles or a man who does not produce any sperm. Sterility occurs in 3–5 percent of couples.[3] Infertility, on the other hand, is an inability to conceive for one to two years by a couple who are having acts of unprotected sexual intercourse during the woman’s fertile days.[4] From 10–15 percent of married couples are infertile.[5] The incidence of infertility increases with age, particularly of the female partner. Three national US surveys found that 7 percent of couples whose female partners were aged 20–4 years were infertile, 9 percent for those aged 25–9, 15 percent for those aged 30–4 years, 22 percent for those aged 35–9, and 29 percent for those aged 40–4 years.[6] Infertility statistics include cases of tubal ligation and vasectomy. While the normal monthly fertility rate ranges from 15 to 20 percent, subfertile couples where the woman is less than 30 years of age may have a monthly fertility rate of 4—5 percent for up to 3 years.[7]
The causes of a couple’s infertility may be in one or both partners. A woman may fail to ovulate due to a hormonal disorder or because of polycystic ovary syndrome. Occasionally a superfertile partner can make up for what is lacking in a subfertile partner.
The causes of infertility among couples who presented for infertility treatment in Australia and New Zealand in 1997 were tubal 12 percent, male factor 33 percent, endometriosis 6 percent, other causes 9 percent, multiple causes 27 percent, and unexplained 13 percent.[8] But the rates for tubal and male factors for 1979–95 were 34 percent and 19 percent respectively. The increase in male infertility in 1997 explains the drop in the percentage for tubal causes.[9] In the UK single and multiple causes of female infertility in all treatment cycles were tubal disease 36 percent, endometriosis 8 percent, unexplained 45 percent, and other 19 percent.[10] Stress is also a seasonal factor that adversely affects female fertility.[11] Although one cause of infertility may be dominant, often more than one factor may affect a couple’s fertility.
In the USA it has been suggested that female infertility is caused by failure to produce fertile eggs in 10–15 percent of cases and by pelvic factors like endometriosis, infection, or tubal blockage in 30–40 percent of cases. Education could prevent, or at least minimize, female infertility caused by infection associated with sexually transmitted diseases. Some women fail to ovulate as a result of chemotherapy, surgery or other causes. Others do not want to use their own eggs if they are carriers of a serious inherited disorder such as hemophilia. In these cases recourse to donor eggs is less frequent if use is made of preimplantation genetic diagnosis (PGD) which enables couples to select and implant only their own healthy genetic embryos. Male infertility is caused in 30–40 percent of cases by low sperm count (less than 20 million sperm per ml. of semen), low motility, high viscosity of semen, or insufficient semen. A further 10–15 percent of infertility is caused by sperm being impeded from penetrating cervical mucus. The cause of infertility is unknown in about 10 percent of couples.[12]
The sperm count in men is falling at an alarming rate of >2 percent every year. The evidence indicates the likely causes are the effects of environmental chemicals, e.g. pesticides, on the human reproductive system and xeno-estrogens which imitate the action of the female hormone estrogen on male reproductive health.[13] However, an increase in couple fertility compensates for any decline in male fertility.[14] There is also evidence of increased mutations in sperm and of more genetic defects in the children of older fathers.[15] The paternal-age effect is less frequent than the maternal-age effect and is more likely to involve inheritable mutation disorders or sex chromosome errors, while the maternal-age effect is more likely to be associated with increased risks of obstetrical complications, perinatal problems or autosomal trisomies.[16]
[6.1.2]
Treatment
It frequently happens that women who have been unable to conceive for more than a year, become pregnant while awaiting treatment. Some women who have been using contraceptive pills for years may not need treatment, but simply more time for the resumption of ovulation. These possibilities need to be ruled out before undergoing infertility treatment. For some whose work times permit it, all that is needed is for the couple to make use of “timed intercourse” to coincide with natural ovulation.[17] Though infertility is more akin to a disability than a disease, most infertile couples need medical treatment after 12 months of unsuccessful attempts to conceive.[18]
Where there are ovulation defects, or the cause of infertility is unknown, ovulation induction may be used with a mild stimulation protocol of superovulation hormones under controlled conditions. Fertilization may then occur following artificial intrauterine insemination and/or normal sexual intercourse, with a pregnancy rate up to 33 percent.[19] Blocked fallopian tubes can also be treated by microsurgery with subsequent intrauterine pregnancy rates from about 25–50 percent within two years.[20] Microsurgery is not very effective for women who have been sterilized by cauterization due to the width of destruction of the fallopian tubes. After female sterilization with clips, microsurgical reversal is successful in up to 80 percent of cases. Unsuccessful attempts of reversal of vasectomy is a frequent cause of male infertility.[21]
The most frequently used infertility treatment procedure is the insemination of eggs by sperm by IVF followed by embryo transfer to the uterus (ET). Semen may be collected following sexual intercourse and be treated to make it less viscous and sperm more motile. The sperm and eggs, separated by an air bubble, may then be placed in a catheter and promptly injected into the fallopian tube where conception occurs. This procedure is known as gamete intra fallopian transfer (GIFT). Sperm can also be injected under the zona pellucida of the egg to enable fertilization to occur later on when the membranes of sperm and egg fuse. This is called subzonal insemination (SUZI) and may be performed in a way similar to GIFT.
[1] Tara Hurst et al., Assisted Conception, Australia and New Zealand, 1997. AIHW cat. no. PER 10 (Sydney: Australian Institute of Health and Welfare National Perinatal Statistics Unit, 1999, Assisted Conception Series no. 4), 1.
[2] See Karen Dawson, Reproductive Technology: The Science, the Ethics, the Law and the Social Issues (Melbourne: VCTA Publishing, Macmillan Education Australia, 1995); D. M. Saunders and L. J. Satchwell, Assisted Reproductive Technology: What the doctor should know (New York & London: The Parthenon Publishing Group, 1995); Donald Evans and Neil Pickering, eds., Creating the Child: The Ethics, Law and Practice of Assisted Procreation (The Hague: Martinus Nijhoff Publishers, 1996)
[3] Egbert te Velde et al., “Variation in Couple Fecundity and Time to Pregnancy, An Essential Concept of Human Reproduction,” Lancet 355 (2000): 1928-9.
[4] Ibid., 1928–9; J. Yovich and G. Grundzinskas, “The Spectrum of Infertility,” The Management of Infertility: A Manual of Gamete Handling Procedures (Oxford: Heinemann, 1990), 5–11.
[5] Dawson, Reproductive Technology, 1–2.
[6] D. R. Mishell and V. Davajan, “Evaluation of the Infertile Couple,” in D. R. Mishell et al., Infertility, Contraception and Reproductive Endocrinology, 3rd ed. (Boston: Blackwell Scientific Publications, 1991), 557–9.
[7] Egbert te Velde and Bernard J. Cohlen, “The Management of Infertility,” New England Journal of Medicine 340 (1999): 224.
[8] Hurst et al., Assisted Conception, 41.
[9] Ibid., 9, 41.
[10] Human Fertilization and Embryology Authority (HF&EA). Seventh Annual Report & Accounts 1998, 8.
[11] Peter T. Ellison, “Human Ovarian Function and Reproductive Ecology: New Hypotheses,” American Anthropologist 92/4 (1990): 933–52.
[12] Mishell, “Evaluation of the Infertile Couple,” 562; Dawson, Reproductive Technology, 1, 5–15.
[13] Louise Vandelac and Marie-Helene Bacon, “Will We Be Taught By Our Clones? The Mutations of the Living, From Endocrine Disruptors to Genetics,” Bailliere’s Clinical Obstetrics and Gynaecology 13/4 (1999): 581–3; Alfred Spira and Luc Multigner, “The Effect of Industrial and Agricultural Pollution on Human Spermatogenesis,” Human Reproduction 13/8 (1998): 2041-2.
[14] Michael Joffe, “Time Trends in Biological Fertility in Britain,” Lancet 355 (2000): 1961-5.
[15] E. L. Yong et al., “Male Infertility and the Androgen Receptor: Molecular, Clinical and Therapeutic Aspects,” Reproductive Medicine Review, 6 (1997): 113–31; M. Auroux, “Age of the Father and Development,” Contraception, Fertility, Sexualite 21 (1993): 382–5.
[16] Juan J. Tarin et al., “Long-term Effects of Delayed Parenthood,” Human Reproduction 13/9 (1998): 2371–6; A. J. Wyrobek et al., “Mechanisms and Targets Involved in Maternal and Paternal Effects on Numerical Aneuploidy,” Environmental and Molecular Mutagenesis 28/3 (1996): 254–64.
[17] See Infertility: Guidelines for Practice, Fertility Committee of the Royal College of Obstetricians and Gynaecologists (London: RCOG Press 1992).
[18] Swren Holm, “Infertility, Childlessness and the Need for Treatment,” in Evans and Pickering, Creating the Child, 65–78; R. G. Edwards, “Human Conception in vitro 1995, a Summing Up,” Human Reproduction 11 Suppl 1 (1996): 199-211.
[19] David S. Guzick et al., “Efficacy of Superovulation and Intrauterine Insemination in the Treatment of Infertility,” New England Journal of Medicine 340 (1999): 177–83; te Velde and Cohlen, “The Management of Infertility,” 225.
[20] Michael G. R. Hull and Charlotte E Fleming, “Tubal Surgery Versus Assisted Reproduction: Assessing their Role in Infertility Therapy,” Current Opinions in Obstetrics and Gynecology 7 (1995): 161.
[21] Dawson, Reproductive Technology, 9.
2.
DIGNITAS
PERSONÆ
on INFERTILITY
and MEDICAL
TREATMENT
|
Second Part: |
PARS II |
|
New Problems Concerning Procreation |
NOVAE QUAESTIONES DE PROCREATIONE |
|
11. In light of the principles recalled above, certain questions regarding procreation which have emerged and have become more clear in the years since the publication of Donum vitae can now be examined. |
11. Spectatis principiis supra memoratis oportet nunc diiudicare de quibusdam quaestionibus procreationem spectantibus. quae in lucem prodierunt et clariore forma ditatae sunt in annis post publici iuris faetam Instructionem Donum vitae |
|
Techniques for assisting fertility |
Technicae methodi adiuvantes fertilitatem |
| 12. With regard to the treatment of infertility, new medical techniques must respect three fundamental goods: | 12. Quoad curam infertilitatis. novae artes technicae medicinae debent observare tria fundamentalia bona: |
|
a) the right to life and to physical integrity of every human being from conception to natural death; |
a) ius ad vitam et ad physicam integritatem humanae cuiusque creaturae inde a conceptione usque ad mortem naturalem; |
|
b) the unity of marriage, which means reciprocal respect for the right within marriage to become a father or mother only together with the other spouse; [19DonVit II,A,1] |
b) matrimonii unitatem, quae secumfert mutuam observantiam coniugum iuris, ut pater et mater fieri valeant solummodo alter per alterum;19 |
|
c) the specifically human values of sexuality which require “that the procreation of a human person be brought about as the fruit of the conjugal act specific to the love between spouses”.[ 20DonVit II,B,4] |
c) sexualitatis valores potissimum humanos, qui «poscunt ut humanae personae procreatio habeatur veluti fructus actus coniugalis, qui est nota propria mutui coniugum amoris»20 |
|
Techniques which assist procreation “are not to be rejected on the grounds that they are artificial. As such, they bear witness to the possibilities of the art of medicine. But they must be given a moral evaluation in reference to the dignity of the human person, who is called to realize his vocation from God to the gift of love and the gift of life”. [21DonVit Intr. 3] |
Interventus technici. qui adiutorio sunt procreationi «quatenus artificiosi. respuendi non sunt. Qua tales testantur quid valeat ars medica; at eorum moralis aestimatio referatur oportet ad dignitatem humanae personae, cuius est perficere divinam sibi inditam vocationem ad donum amoris atque ad donum vitae».21 |
|
In light of this principle, all techniques of heterologous artificial fertilization,22 as well as those techniques of homologous artificial fertilization23 which substitute for the conjugal act, are to be excluded. |
Sub lumine huiusmodi criterii nequeunt omnino adhiberi teehnicae quaeque artes fecundationis artificiosae heterologae 22 necnon technicae artes fecundationis artificiosae homologae 23 actum coniugalem subrogantes. |
|
22 The term heterologous artificial fertilization or procreation refers to “techniques used to obtain a human conception artificially by the use of gametes coming from at least one donor other than the spouses who are joined in marriage” (Instruction Donum vitae, II: AAS 80 [1988], 86). 23 The term homologous artificial fertilization or procreation refers to “the technique used to obtain a human conception using the gametes of the two spouses joined in marriage” (Instruction Donum vitae, II: AAS 80 [1988], 86). |
|
|
On the other hand, techniques which act as an aid to the conjugal act and its fertility are permitted. The Instruction Donum vitae states: “The doctor is at the service of persons and of human procreation. He does not have the authority to dispose of them or to decide their fate. A medical intervention respects the dignity of persons when it seeks to assist the conjugal act either in order to facilitate its performance or in order to enable it to achieve its objective once it has been normally performed”.24 |
Permittuntur econtra technicae artes, quae speciem habeant auxilii ad actum coniugalem rite explendum atque ad eiusdem fecunditatem.. Instructio Donum vitae ita docet: «Medicus munere fungitur deserviendi bono personarum et humanae procreationi; quoad haec, ille nec disponendi nec decernendi potestatem habet. Medicus interventus tunc personarum dignitatem tuetur. cum actum coniugalem adiuvare studet, sive ut facilius expleatur, sive ut idem, iam rite expletus. finem suum assequi possit ».24 |
|
24 CDF Donum vitae, II, B, 7: AAS 80 (1988), 96; cf. Pius XII, Address to those taking part in the Fourth International Congress of Catholic Doctors (29 September 1949): AAS 41 (1949), 560. |
|
|
And, with regard to homologous artificial insemination, it states: “Homologous artificial insemination within marriage cannot be admitted except for those cases in which the technical means is not a substitute for the conjugal act, but serves to facilitate and to help so that the act attains its natural purpose” 25 [DonVit II,B,6] |
Atque item de inseminatione artificiosa homologa, docet: « seminatio artificialis homologa intra ambitum matrimonii admitti nequit, excepto casu in quo apparatus technicus non sit substitutivus actus coniugalis, sed se praebeat ut adiumentum ad naturalem eius finem facilius assequendum ».25 |
| 13. Certainly, techniques aimed at removing obstacles to natural fertilization, as for example, | 13. Licite procul dubio adhiberi possunt interventus apti ad removenda fertilitatis naturalis impedimenta. ut sunt, exempli gratia, |
|
hormonal treatments for infertility, surgery for endometriosis, unblocking of fallopian tubes or their [micro-]surgical repair, |
cura hormonalis infertilitatis quae oriatur a gonadibus, cura chirurgica endometriosis, tubarum obstructionis sanatio, vel microchirurgica tubarum pervietatis restauratio. |
|
are licit. All these techniques may be considered authentic treatments because, once the problem causing the infertility has been resolved, the married couple is able to engage in conjugal acts resulting in procreation, without the physician’s action directly interfering in that act itself. None of these treatments replaces the conjugal act, which alone is worthy of truly responsible procreation. |
Omnes huiusmodi technicae artes haberi possunt germanae therapiae. quatenus, amotis impedimentis quae prima causa fuerint infertilitatis, coniuges aetus ponere possint cum felici procreationis exitu, quin medico directe interveniendum sit in ipso coniugali actu; etenim harum technicariun rationum nulla surrogat coniugalem actum, qui unus exstat dignus procreationis plene consciae. |
|
In order to come to the aid of the many infertile couples who want to have children, adoption should be encouraged, promoted and facilitated by appropriate legislation so that the many children who lack parents may receive a home that will contribute to their human development. In addition, research and investment directed at the prevention of sterility deserve encouragement. |
Ut nonnullorum desiderio praeterea coniugum sterilium subveniatur, ardenter filium affectantium, optandtum est ut foveatur, promoveatur et facilior reddatur, opportunis legibus. ratio de adoptione innumerorum exstantium puerorum orphanorum. qui domestica domo indigent, ad aptam suam assequendam humanam evolutionem. Demum declarandum est quod cohortatione fovendi sunt quotquot inquirant et opes impendant ad sterilitatempraecavendam aptas |
3. NAPROTECHNOLOGY:
An Example of Catholic Infertility-Research
http://www.naprotechnology.com/
http://www.popepaulvi.com/
Until 1978, most of the effort in medicine in evaluating and treating women with infertility was placed in trying to identify and treat the underlying causes. In 1978, in vitro fertilization produced a paradigm shift. It led to a “skipping over” the causes and this continues up to the present time to be the foundational management approach. In essence, this is a symptomatic or Band-Aid approach to treatment, not one that gets to the root causes. When the artificial reproductive technologies began to take hold, now over 25 years ago, diagnostic laparoscopy was in its infancy. Hormone assessment, while available, was not readily accessible. Ultrasound technology was still mired in sector scanning and real-time ultrasonography was not yet available. Selective hysterosalpingography had not yet been developed and the fallopian tubes could not be catheterized. The Creighton Model FertilityCare™ System began its first Allied Health Education Program for FertilityCare™ Practitioners (FCP) in 1978. This means of objectively monitoring the biomarkers of the menstrual and fertility cycle was only in its beginning stages. With the availability of the CrMS, observations of mucus patterns during the course of the menstrual and fertility cycle could be observed for the very first time. In fact, information obtained by women charting their cycles in this fashion is unique and can only be obtained in this fashion.
The Goals of NaProTECHNOLOGY in Infertility
A NaProTECHNOLOGY approach to the infertile couple has the following goals:
In Figure 51-38, a comparison is made of the “per woman” pregnancy rates between the NaProTECHNOLOGY approach and in vitro fertilization. This study shows that a NaProTECHNOLOGY approach for women who have anovulatory infertility, polycystic ovarian disease, endometriosis, or tubal occlusion, all have statistically significantly higher pregnancy rates than patients with similar conditions treated with in vitro fertilization.
[Figure 51-38, p. 691 from the NaPro textbook. The “per woman” pregnancy and
family-building rates comparing NaProTECHNOLOGY and in vitro fertilization
(From: Pope Paul VI Institute research, 2004 and the listed references).]
4.
4. DEBATED
TREATMENTS:
G.I.F.T.
|
|
Four-month old human fetus |
From the Bioethics Center at Loras College, Debuque, Iowa. [webpage no longer available]
The assisted reproductive technology of Gamete Intrafallopian Transfer (GIFT) involves three steps.
|
1. THE FIRST STEP |
|
|
|
Medications are used to stimulate the woman to produce more than one follicle and ovum, and to aid in stimulating the follicles to release the ova. During this time the woman’s response to the medication and the development of her ova are watched and assessed.
|
2. THE SECOND STAGE |
begins with a laparoscopy performed under general anesthesia to retrieve the ova. The ova are then examined under a microscope to determine maturity. Semen is obtained and processed in a centrifuge, where it is washed and then placed in a test tube so that the active sperm can swim to the top.
|
|
|
|
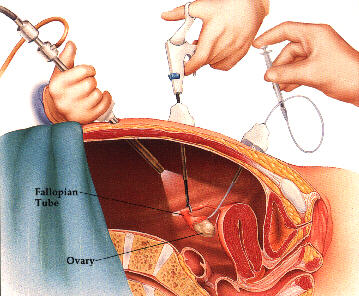
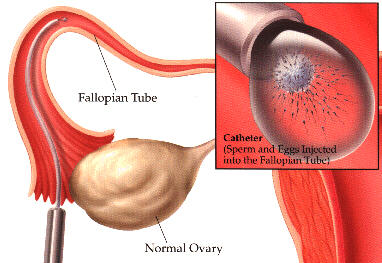
3. THE THIRD STEP |
consists in transfer of the ova and sperm into the woman's body. Ova and sperm are placed in a catheter, and the catheter is inserted directly into the woman’s fallopian tube through a surgical procedure using a laparoscope. The ova and sperm are then injected into the fallopian tube, with the intent of fertilization occurring in its normal environment within the woman’s body. If fertilization does occur, the developing embryo(s) will remain in the fallopian tube and then move to the uterus for implantation.
Policy
The use of Gamete Intrafallopian Transfer (GIFT) by marital spouses is not excluded, provided that the following restrictions are observed:
1) the retrieval of ova and sperm must follow a natural act of sexual intercourse;
2) sperm must be collected from that act of intercourse by morally acceptable means;
3) the procedure must be carried out in such a way as to avoid the possibility of extracorporeal conception;
4) any ova collected but not transferred back into the woman?s body must not be fertilized in vitro, with the resulting embryos frozen for later implantation.
Should a multifetal pregnancy result through the use of the GIFT procedure, pregnancy reduction, that is, the abortion of some of the fetuses, is not permissible.
Sources of Policy
The Instruction on Respect for Human Life in
its Origin and On the Dignity of Procreation from the Vatican Congregation
for the Doctrine of the Faith (1987) did not explicitly pass judgment on the
GIFT procedure. (2) Cardinal Joseph Ratzinger, prefect of the Congregation for
the Doctrine of the Faith at the time the Instruction was issued, gave
the following instructions on techniques whose use had been left open: ?When the
discussion is still open and there is not yet a decision by the
magisterium, the doctor is required to stay informed, according to classic
theological principles and concrete circumstances? and to ?make a decision based
on his informed conscience.? (3)
The following directives from the Ethical and Religious Directives for Catholic Health Care Services, based on the Vatican Instruction, are relevant to assessing the moral permissibility of the GIFT procedure:
When the marital act of sexual intercourse is not able to attain its procreative purpose, assistance that does not separate the unitive and procreative ends of the act, and does not substitute for the marital act itself, may be used to help married couples conceive. (no. 38)
41. Homologous artificial fertilization (that is, any technique used to achieve conception using the gametes of the two spouses joined in marriage) is prohibited when it separates procreation from the marital act in its unitive significance (e.g., any technique used to achieve extra-corporeal conception). (no. 41) (4)
The restriction concerning the method of collecting sperm is derived from the Church?s long-standing teaching on the immorality of masturbation. This teaching was reaffirmed in 1975 by the Sacred Congregation for the Doctrine of the Faith in the Declaration on Certain Problems in Sexual Ethics:
...both the magisterium of the Church, in the course of a constant tradition, and the moral sense of the faithful have been in no doubt and have firmly maintained that masturbation is an intrinsically and gravely disordered action. The principal argument in support of this truth is that the deliberate use of the sexual faculty, for whatever reason, outside of marriage is essentially contrary to its purposes. For it lacks that sexual relationship demanded by the moral order and in which ?the total meaning of mutual self-giving and human procreation in the context of true love? is achieved. All deliberate sexual activity must therefore be referred to the married state. (5)
Regarding the third restriction, see the handbook entries on In Vitro Fertilization (IVF) and Cryopreservation (Freezing) of Embryos.
The prohibition against selective reduction is part of the Church?s unqualified opposition to direct abortion; see the Congregation for the Doctrine of the Faith, Declaration on Procured Abortion (1974). (6)
1. Fertilitext, Gamete Intrafallopian Transfer (GIFT), http://www.fertilitext.org/gift.html; FertilityRX.com, Assisted Reproductive Technology, Section IV: Gamete Intrafallopian Transfer (GIFT), http://iop.com/ ~poetsrx/art/gift.html; Reproductive Medicine Group, Tampa, FL, Gamete Intrafallopian Transfer (GIFT), http://www.vbtivf.com/GIFT.htm; Lycos Health by WedMD, Gamete Intrafallopian Transfer (GIFT), and Zygote Intrafallopian Transfer (ZIFT), http://webmd.lycos.com/content/dmk/dmk_article_5461649; Am-I- Pregnant.com, Gamete/Zygote Intrafallopian Transfer, GIFT, http://www.am-i-pregnant.com/giftinv.shtml.
2. Congregation for the Doctrine of the Faith, Instruction on Respect for Human Life in its Origin and On the Dignity of Procreation (Donum Vitae) (Washington, DC: United States Catholic Conference, 1987).
3. Origins 16/40 (March 19, 1987): 697, 699-11 at 699, marginal notes.
4. National Conference of Catholic Bishops, Ethical and Religious Directives for Catholic Health Care Services (1994) (Washington, DC: United States Catholic Conference, 1995).
5. Sacred Congregation for the Doctrine of the Faith, Declaration on Certain Problems of Sexual Ethics (Dec. 29, 1975), no. 9, reprinted in Kevin D. O?Rourke , OP and Philip Boyle, OP, Medical Ethics Sources of Catholic Teachings (St. Louis: Catholic Health Association, 1989).
6. Reprinted in Austin Flannery, O.P. (ed.), Vatican Council II: More Post Conciliar Documents, vol. 2 (Northport, NY: Costello Publishing Company, 1982).
COMMENTARY
GAMETE INTRAFALLOPIAN TRANSFER (GIFT)
Medical Facts about GIFT
The GIFT procedure was developed in 1984 by Dr. Ricardo Asch and his associates at the University of Texas Health Science Center in San Antonio. (1) The procedure is 'most often recommended for couples with unexplained infertility with the female partner having at least one open fallopian tube.' (2) It can also be recommended 'for patients whose infertility is due to cervical or immunological factors, mild endometriosis, or selected cases of male infertility.' (3)
GIFT is considered a variation of in vitro fertilization (IVF), with one significant difference. With the GIFT procedure, it is intended that fertilization occur naturally within the woman's body instead of in a laboratory. (4) For this reason, GIFT is sometimes described as 'an alternative for patients whose religious beliefs prohibit conception outside the body.' (5)
Reports of the success rate of GIFT in comparison with IVF vary. Some reports indicate a higher successs rate for GIFT in achieving a pregnacy. (6) Other reports indicate similar success rates for GIFT and IVF (7), with IVF supplanting GIFT at some fertility clinics. (8)
A procedure called Tubal Ovum Transfer (TOT), or alternately, Tubal Ovum Transfer with Sperm (TOTS) is very similar to GIFT and has been superseded by it. (9)
Theological Opinion about GIFT
The Pope John Center, in consultation with Msgr. Carlo Caffarra, head of the Pope John Paul II Institute for the Family in Rome, approved the GIFT procedure in 1985, with the restriction that sperm are collected during an act of sexual intercourse. (10) However, the legitimacy of the GIFT procedure was not accepted by all theologians, and the controversy continued through the decade of the 1990's. (11) Nevertheless, the GIFT procedure has not, to date, been explicitly rejected by the magisterium. (12) Because of the lack of agreement among reputable theologians, and concomitantly, because of the lack of an explicit pronouncement of approval by the magisterium, the handbook's policy statement is stated cautiously, namely, that the use of GIFT by marital spouses is not excluded. (13)
Defense of the Permissibility of the GIFT Procedure
Rev. Donald McCarthy of the Pope John Center has defended the GIFT procedure on the following grounds:
The conjugal act in the described procedure remains the essential step in getting the ovum and sperm to meet. This step is followed by the repositioning of the ovum and sperm in a manner which markedly increases the likelihood of fertilization. Hence, GIFT...can be seen as a medical procedure which assists, rather than replaces, the conjugal act...
In conclusion, while the GIFT technique uses technology to assist fertilization, it simply re- positions the sperm and ova to enhance the desired outcome of fertilization. The link between the marital act and procreation is realized by technical assistance. (14)
It should be noted that there is theological precedent for regarding the repositioning of ova or sperm after an act of sexual intercourse as morally permissible; see the entry Theological Opinion on Permissible Assisted Reproductive Technologies (ARTs). GIFT likewise involves the temporary exteriorization of ova and the temporary exteriorization and processing of sperm after an act of sexual intercourse. Again, there is theological precedent for regarding these procedures are morally permissible; see the entry Theological Opinion on Permissible Assisted Reproductive Technologies (ARTs).
Further, Peter Cataldo has attempted to spell out more exactly what it means for a technological procedure to replace the conjugal act or to assist it:
A procedure replaces the conjugal act if it determines, of itself, those conditions which immediately secure the success of fertilization; a procedure assists the conjugal act if it does not determine, of itself, those conditions which immediately secure the success of fertilization, but rather allows fertilization to take place under immediate conditions which are natural. (15)
Using this criterion, Cataldo argues that GIFT is a morally legitimate procedure:
...I believe that GIFT with a conjugal act assists that act because the immediate conditions of fertilization are not determined or created by the procedure itself. Unlike IVF and the other procedures which replace the conjugal act, fertilization itself takes place in GIFT within natural conditions which are essentially the same as those in which a pathology is not present. (16)
Central Objection to the GIFT Procedure
The central objection voiced against the GIFT procedure is that it does not really assist an act of sexual intercourse, but rather, illegitimately substitutes for the conjugal act between spouses in achieving conception. This objection has been developed in several ways.
William May contends that this procedure makes the conjugal act incidental to the achievement of pregnancy in that an act of sexual intercourse is needed only to obtain sperm in a morally acceptable way:
...I think it must be said that in the GIFT procedure the conjugal act is in truth incidental and not essential to the achievement of pregnancy. The bond between the marital act and the GIFT procedure is not essential. This is quite obvious from the fact that this procedure as such does not require the marital act. There is a complete dissociation between the marital act and the technical method which leads to conception. The only reason to engage in the marital act is to obtain the husband's sperm in a non-masturbatory way. But this is only incidental to the GIFT procedure as such. ...GIFT, therefore, substitutes for the marital act as far as the conception of the child is concerned and does not facilitate it or help it to achieve its natural objectives. (17)
Donald DeMarco also contends that these procedures make 'the conjugal act...incidental to the achievement of pregnancy' because 'the technical method could be employed in the complete absence of the sex act, or even of love and marriage.' (18) Indeed, some fertility clinics make explicit that sperm for the procedure is usually obtained through masturbation. (19)
Those approving of the GIFT procedure have pointed out that, when the procedure is employed together with the collection of sperm in a perforated condom during an act of sexual intercourse, some sperm does enter the body of the woman, and hence that the possibility does exist that actual fertilization occurs from that sperm. (20) This possibility is used to counter the charge that GIFT makes the conjugal act purely incidental to the achievement of pregnancy.
Another version of the objection that the GIFT procedure substitutes for the act of sexual intercourse between spouses is developed by John Hass:
With all the procedures which intervene between intercourse and conception in GIFT an integral link between the marital act and procreation is lost. In other words, there is no longer an inherent, necessary and intelligible link between the marriage act and procreation. (21; italics added)
However, it is not simply the passage of time between coitus and the injection of the gametes which would seem to render GIFT immoral but the fact that the intrinsic link between coitus and new life is broken by the intervening human acts. It would seem that the new life is more the result of the actions of technicians and medical personnel rather than the act of love between a husband and a wife. ...What is morally relevant is that the interventions of the technicians and substitution of a host of procedures come to replace the marital act. (22; italics added)
In sum, 'opposition to the moral acceptability of GIFT is based on the reason that the number of interventions breaks the intrinsic link between marital coitus and new life.' (23; italics added)
Peter Cataldo has offered the following reply to this line of argument:
The same procedures considered individually and apart from GIFT are found morally wrong within GIFT. The following interventions taken singly (and in conjunction with the conjugal act) are considered licit as means to overcome infertility: collecting semen with a perforated Silastic sheath; placing it in a syringe, injecting semen into the uterus, treating the sperm, the use of ovulatory drugs, laparoscopic retrieval of eggs, and injection of eggs into the fallopian tubes at an atypical site. Thus, what are considered individually licit interventions become illicit in GIFT because there are too many of them. It is the number as such, the total number of interventions, which is found objectionable. Further proof of this is seen from the fact that the very thing which makes each intervention licit individually is that each does not violate the intrinsic link between conjugal act and procreation. If the very thing needing to be preserved is preserved individually by each, then the reason for the rejection of those same procedures must be the size of their number taken in combination.
Hence, there must be some threshold number which makes the moral difference between assistance and replacement for those who disapprove of GIFT. But what is that number, and how is it to be determined' In fact, there cannot be such a threshold because it cannot be objectively determined. Moreover, Donum Vitae does not place an inherent, quantitative limit to the concept of assistance. The number of steps in between conjugal act and fertilization is not morally decisive for the difference between assistance and replacement... (24)
In further defense of the union between the couple's act of sexual intercourse and conception it might be recalled that fertilization is not simultaneous with the act of intercourse, but is a process that can take up to thirty hours. (25) Indeed, there are cases where fertilization does not begin until two or three days after intercourse because the woman has not yet ovulated and because the sperm still have sufficient viability to bring about fertilization. (26)
Yet a third version of the objection has been presented by Benedict Ashley and Kevin O'Rourke:
We agree, however, with DeMarco that even if fertilization is not extracorporeal, the ethical defect of GIFT is that fertilization is not directly the result of the marital act, since the semen used is not deposited by that act in the vagina, but by a technician's manipulation which substitutes for the marital act... Hence, 'the immediate condition by which fertilization takes place' it seems to us is not the marital act but the technician's manipulations. Nor is it relevant to cite as a precedent the traditional statement of the moral manuals, for which also Pius XII made allowances, that it would be permissible (if it were shown to be effective, which seems not to be the fact) for the husband to use some device to move semen higher into the vagina or uterus to enhance the possibility of conception. In that case it was supposed that the semen was deposited in the vagina of the woman by normal intercourse and remained within her. (27)
Those approving of the GIFT procedure might again point out that, when the procedure is employed together with the collection of sperm in a perforated condom during an act of sexual intercourse, some sperm does enter the body of the woman, and hence that the possibility does exist that actual fertilization occurs from that sperm. (28)
Extracorporeal Conception and the GIFT Procedure
When the GIFT procedure was initially developed, the protocol included air spaces between the sperm and ova when they were placed in the catheter for insertion into the woman's body. This was done in order to keep them separated and to prevent fertilization outside the body. (29) This respected the Catholic view that extracorporeal conception is not morally permissible. (30)
While some fertility clinics have retained this protocol (31), a number of descriptions of the GIFT procedure now speak of the sperm and ova being "placed together" or "mixed" during the step of transferring them into the woman's fallopian tube. (32) At the same time, it is affirmed that fertilization takes place in the normal, natural way within the woman's body in her fallopian tube. (33) Indeed, GIFT is described as 'an alternative for patients whose religious beliefs prohibit conception outside the body.' (34)
Once sperm and ova are in contact, how can it be claimed unequivocally that fertilization takes place within the woman's body' Here it might be replied that "fertilization is a series of processes rather than a single event.' (35) Specifically, fertilization involves penetration of the corona radiata, attachment to and penetration of the zona pellucida, fusion of sperm and egg, prevention of polyspermy, metabolic activation of the egg, decondensation of the sperm nucleus, completion of meiosis in the egg, and the development and fusion of male and female pronuclei. (36) The short time in which ova and sperm are mixed extracorporeally while being transferred into the woman's body during the GIFT procedure, combined with the temporal series of events needed for fertilization, may well undergird the claim that fertilization takes place in the natural way in the woman's fallopian tube in this procedure.
Nevertheless, as a mattter of moral caution, Catholic couples seeking to use the GIFT procedure are encouraged to inquire how it is being performed at that particular fertility clinic and to request the original protocol in which air spaces are included between the sperm and ova when they are placed in the catheter for insertion into the woman's body. The original protocol is a simple one, and it should not be a burden on the clinic to carry out the procedure in this way.
1. MALE
INFERTILITY
and the
PHTHALATE
CONTROVERSY
A recent study out of the University of
Massachusetts found that phthalates in plastics and male infertility may be
connected at the very earliest stages of conception when embryos form during IVF.
Phthalates are the chemicals that give plastic products strength and
flexibility, and have been shown to interfere with the endocrine system in both
men and women. Hundreds of products contain these compounds, including shampoo
bottles, raincoats, flooring and garden hoses.
https://uscfertility.org/plastics-male-infertility/#:~:text=A%20recent%20study%20out%20of,when%20embryos%20form%20during%20IVF.&text=The%20study%20tracked%20through%20urinalysis,to%20begin%20an%20IVF%20cycle
|
|
|
MALE INFERTILITY / PHTHALATE CONTROVERSY |
“Serum estradiol levels in infertile men with
non-obstructive azoospermia”
Nader Salama and Saeed Blgozah
Therapeutic Advances in Reproductive Health, vol. 14, June 18, 2020
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7325549/
|
|
|
Estradiol |
Recently,
exposure to estrogen has become inflated. These estrogens have become ubiquitous
during the normal daily life of most people. A list of estrogenic compounds such
as medications, chemical pesticides, and even food in the form of phytoestrogens
is growing rapidly.13 This
has prompted several scientific groups to call this rising trend in estrogen
contact estrogenic pollution and warn against it. An ongoing argument has arisen
in many areas of the globe about the probable consequences of this pollution.
Some researchers have incriminated estrogenic pollution in the global decrease
in sperm count in men and the increase in anomalies of the male genital system.14 Others
have disputed these links and indicated that there is a lack of sufficient
evidence.15,16 However,
they could not completely discount the possible association in some vulnerable
populations.16
ON the Respective Roles of Estrogen and Testosterone in the Male Testis
Estrogens play an important role in ensuring proper function of the male reproductive tract. In males, the main biologically active estrogen is estradiol. The primary source of this hormone is from the aromatization of testosterone1. Estrogen receptors alpha and beta (ERα and ERβ), together with the membrane associated G-protein-coupled functional ER (GPER), and the enzyme cytochrome P450 aromatase, which converts testosterone to estrogen, are abundant within the testis2,3,4. Estradiol is produced in immature germ cells, spermatozoa, in the epithelium of the efferent ductules and the proximal epididymal duct and in the Leydig cells and Sertoli cells5,6,7,8,9. Thus, it is possible that estradiol concentrations within the testis and semen can even exceed those found in the female vasculature10,11,12,13,14,15. The function of estradiol varies depending on the cells in which it is being produced. In testicular cells, estradiol is known to regulate numerous aspects of spermatogenesis, including proliferation, differentiation, survival and apoptosis of germ cells16,17,18,19,20. Estradiol is involved in the modulation of cell communication via the tight junctions of Sertoli cells and in the regulation of Leydig cell function21,22,23,24,25. Estradiol has been shown to play a role in proliferation, regulation of ion transport and regulation of apoptosis in Sertoli cells26,27,28. In addition, estradiol is responsible for the inhibition of Leydig cell testosterone production and the blocking of Leydig cell regeneration29,30. In the efferent ductules, estradiol is involved in the reabsorption of fluids, thus, affecting sperm concentration, motility and morphology31. As the regulation of testicular cells by estradiol shows both inhibitory and stimulatory influences, this points to a delicate, dose-dependent and temporally sensitive modulation32.
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2002