|
|
Virgin and Child, Master of Moulins, 1499 |
|
|
|
Virgin and Child, Master of Moulins, 1499 |
|
1. EMBRYONIC DEVELOPMENT; 2. FETAL DEVELOPMENT; 3. VIABILITY; 4. “ABORTION PILL”
PLEASE note that the black-and-white photographs shown here were assembled by the Carnegie Embryology Institute over several decades, beginning in 1914, as part of a national effort to identify, describe, and standardize the stages of human embryological and fetal development. The photographs are of embryos that were the result of spontaneous miscarriages or that were discovered during a necessary hysterectomy. In other words, these are not photographs of intentionally-aborted embryos.
For embryo sizes compared with a US penny:
http://virtualhumanembryo.lsuhsc.edu/HEIRLOOM/Stages/Stages_intro.html
|
|
|
|
|
|
|
WEEK 3 |
|
|
|
|
|
|
|
|
STAGE
11; |
|
|
|
|
|
|
|
|
WEEK 4 |
|
|
|
|
|
|
|
|
STAGE
12; |
|
|
|
|
|
|
|
|
WEEK 5 |
|
|
|
|
|
|
|
|
STAGE
13; |
|
|
STAGE
14; |
|
|
STAGE
15; |
|
|
|
|
|
|
|
|
WEEK 6 |
|
|
|
|
|
|
|
|
STAGE
16; |
|
|
STAGE
17; |
|
|
|
|
|
|
|
|
WEEK 7 |
|
|
|
|
|
|
|
|
STAGE
18; |
|
|
STAGE
19; |
|
|
STAGE
20; |
|
|
STAGE
21; |
|
|
|
|
|
|
|
|
WEEK 8 |
|
|
|
|
|
|
|
|
STAGE
22; |
|
|
STAGE
23; |
|
|
|
|
|
|
|
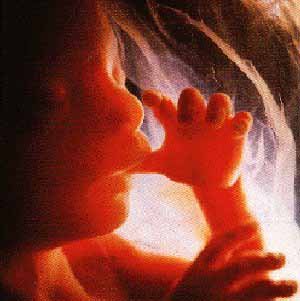
The end of the eighth week marks the END of the “EMBRYONIC PERIOD” and the BEGINNING of the “FETAL PERIOD”.
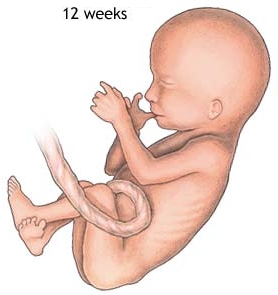
WEEKS 9-12
 |
the fetus reaches a length of 3.2 inches
the head comprises nearly half of the fetus' size
the face is well formed
eyelids close and will not reopen until about the 28th week
tooth buds appear for the baby teeth
limbs are long and thin
the fetus can make a fist with its fingers
genitals appear well differentiated
red blood cells are produced in the liver
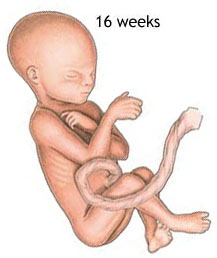
WEEKS 13-16
the fetus reaches a length of about 6 inches
a fine hair develops on the head called lanugo
fetal skin is almost transparent
more muscle tissue and bones have developed, and the bones become harder
the fetus makes active movements
sucking motions are made with the mouth
meconium is made in the intestinal tract
the liver and pancreas produce their appropriate fluid secretions
WEEK 20
 |
the fetus reaches a length of 8 inches
lanugo hair covers entire body
eyebrows and lashes appear
nails appear on fingers and toes
the fetus is more active with increased muscle development
"quickening" usually occurs (the mother can feel the fetus moving)
fetal heartbeat can be heard with a stethoscope
STATISTICS
on VIABILITY
from
Ford, The Prenatal
Person, ch. 9, "Newborns"
Table 9.3: Neonatal intensive care unit, Loyola University Medical Center, survival rates, 1990—4
|
Gestational age, weeks |
Survivors % |
|
22—3 |
19 % |
|
24—5 |
63 % |
|
26—7 |
88 % |
Source: modified from “Neonatal Survival Rates” in Cambridge Quarterly of Healthcare Ethics 8 (1999):162.
Table 9.4: Survival rates by gestational age, 1994–6
|
Gestational age, weeks |
Survivors percentage |
Live births |
|
23 |
35.5 % |
31 |
|
24 |
65.6 % |
36 |
|
25 |
73.9 % |
46 |
|
26 |
85.9 % |
64 |
|
28 |
96.0 % |
75 |
|
32 |
98.1 % |
262 |
Source: modified and calculated from data in the Royal Women’s Hospital in Melbourne, Medical Journal of Australia, June 7, 1999.
WEEK 24
 |
the fetus reaches a length of 11.2 inches
the fetus weighs about 1 lb. 10 oz.
eyebrows and eyelashes are well formed
all the eye components are developed
the fetus has a hand and startle reflex
footprints and fingerprints forming
alveoli (air sacs) forming in lungs
WEEKS 25-28
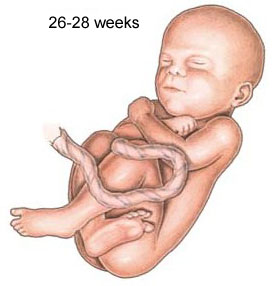
the fetus reaches a length of 15 inches
the fetus weighs about 2 lbs. 11 oz.
rapid brain development
nervous system developed enough to control some body functions
eyelids open and close
respiratory system, while immature, has developed to the point where gas exchange is possible
a baby born at this time may survive, but the possibilities for complications and death remain high
WEEKS 29-32
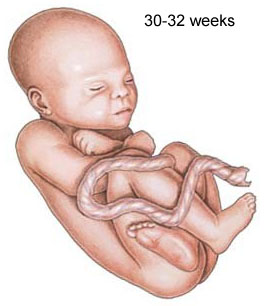 |
the fetus reaches a length of about 15-17 inches
the fetus weighs about 4 lbs. 6 oz.
rapid increase in the amount of body fat
rhythmic breathing movements occur, but lungs are not fully mature
bones are fully developed, but still soft and pliable
fetus begins storing iron, calcium, and phosphorus
WEEK 36
the fetus reaches a length of about 16-19 inches
the fetus weighs about 5 lbs. 12 oz. to 6 lbs. 12 oz.
lanugo begins to disappear
increase in body fat
fingernails reach the end of the fingertips
a baby born at 36 weeks has a high chance of survival, but may require some medical interventions
WEEKS 37-40
considered full-term at 37 weeks
may be 19 to 21 inches in length
lanugo is gone except for on the upper arms and shoulders
fingernails extend beyond fingertips
small breast buds are present on both sexes
head hair is now coarse and thicker
THE
“ABORTION
PILL”
In 2016 the U.S. Food and Drug Administration
approved a two-drug combination of Mifeprex (also called RU-486 or
mifepristone) and Cytotec (commonly known as misoprostol) to induce abortion
without surgery. In 2019 the Centers for Disease Control and Prevention
reported that approximately 42 percent of all abortions in the U.S. were
medication-based.
To start the process, a person takes mifepristone within 10 weeks from their
last period. One or two days later they take misoprostol. Both drugs work
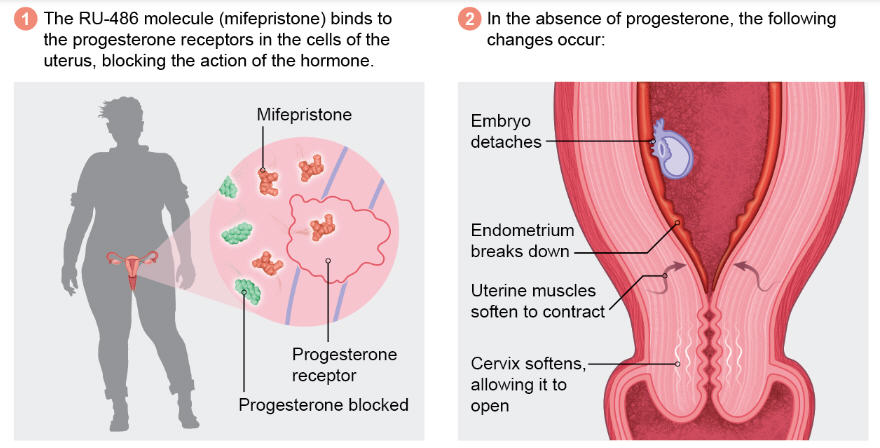
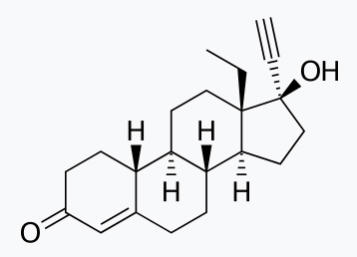
individually, but they are more effective together. Mifepristone blocks
progesterone's action on the uterus, making it incapable of supporting a
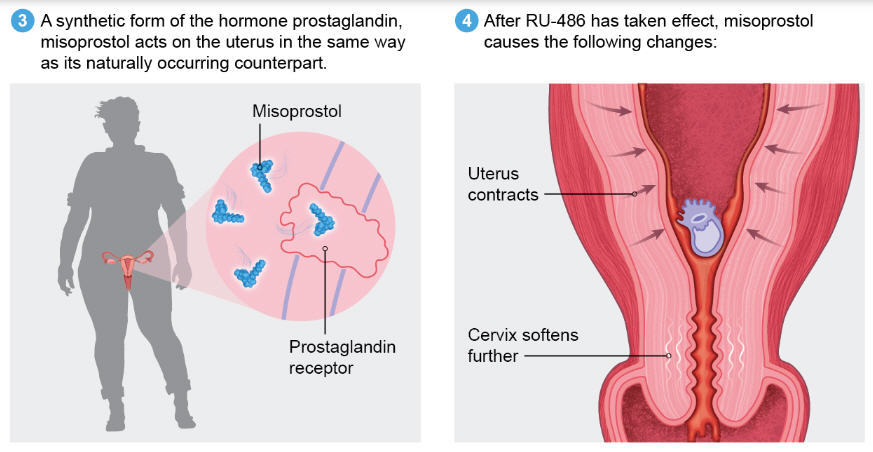
pregnancy. Misoprostol, among other things, starts uterine contractions.
MIFEPRISTONE (RU-486)
EFFECT
|
|
MISOPROSTOL
EFFECT
|
|
|
|
from the PLANNED PARENTHOOD WEBSITE
https://www.plannedparenthood.org/learn/abortion/the-abortion-pill
“Abortion pill” is the common name for using two different medicines to end a pregnancy: mifepristone and misoprostol.
First, you take a pill called mifepristone. Pregnancy needs a hormone called progesterone to grow normally. Mifepristone blocks your body’s own progesterone, stopping the pregnancy from growing.
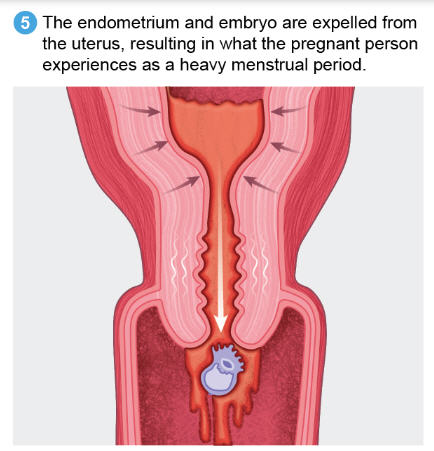
Then you take the second medicine, misoprostol, either right away or up to 48 hours later. This medicine causes cramping and bleeding to empty your uterus. It’s kind of like having a really heavy, crampy period, and the process is very similar to an early miscarriage. If you don’t have any bleeding within 24 hours after taking the second medicine, call your nurse or doctor.
Your doctor or nurse will give you both medicines at the health center. When and where you’ll take them depends on state laws and your health center's policies. Your doctor or nurse will give you detailed directions about where, when, and how to take the medicines. You may also get some antibiotics to prevent infection.
The abortion pill is very effective. The effectiveness depends on how far along you are in your pregnancy when you take the medicine
For people who are 8 weeks pregnant or less, it works about 94-98 out of 100 times.
For people who are 8-9 weeks pregnant, it works about 94-96 out of 100 times.
For people who are 9-10 weeks pregnant, it works about 91-93 out of 100 times. If you're given an extra dose of medicine, it works about 99 out of 100 times.
For people who are 10-11 weeks pregnant, it works about 87 out of 100 times. If you're given an extra dose of medicine, it works about 98 out of 100 times.
The abortion pill usually works, but if it doesn’t, you can take more medicine or have an in-clinic abortion to complete the abortion.
Depending on where you live, you may be able to get a medication abortion up to 77 days (11 weeks) after the first day of your last period. If it has been 78 days or more since the first day of your last period, you can have an in-clinic abortion to end your pregnancy.
DRUGS USED in POST-SEX CONTRACEPTION
DRUGS
USED in
POST-SEX
CONTRACEPTION
The Morning-After Pill
|
|
|
|
LEVONORGESTREL |
ULIPRISTAL |
|
Progestogen (progesterone-like drug)with weak androgenic activity. |
A selective progesterone receptor modulator (SPRM): acts on the progesterone receptor causing different effects in different tissues. |
Both drugs work by blocking or delaying ovulation
and by delaying maturation of the uterine endometrium (lining)
LEVONORGESTREL (Plan B)
Levonorgestrel is a progestogen with weak androgenic activity. It has no other important hormonal activity
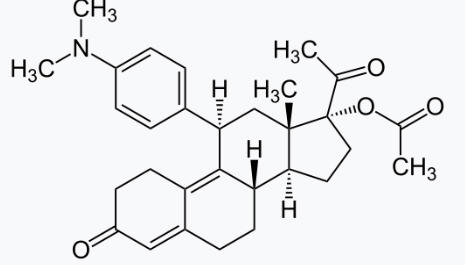
ULIPRISTAL (Ella)
As an SPRM*, ulipristal acetate has partial agonistic as well as antagonistic effects on the progesterone receptor. Ulipristal acetate exhibits similar potency to antagonize progesterone receptor as mifepristone in vitro. Works by blocking or delaying ovulation and of delaying the maturation of the endometrium
*A selective progesterone receptor modulator (SPRM) is an agent that acts on the progesterone receptor (PR), the biological target of progestogens like progesterone. their action differs in different tissues, i.e. agonist in some tissues while antagonist in others. This mixed profile of action leads to stimulation or inhibition in tissue-specific manner
DRUGS
USED to
INDUCE
ABORTION
The Morning-After Pill
|
|
|
|
MIFEPRISTONE |
MISOPROSTOL |
|
Antiprogestogen: progesterone-receptor blocker, causes death and detachment of placenta. |
Prostaglandin: induces uterine contractions |
|
|
|
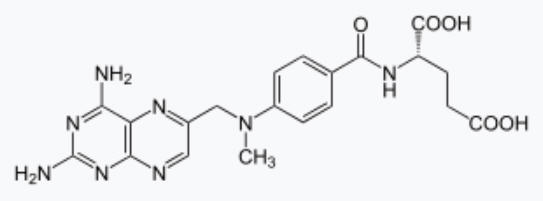
METHOTREXATE |
|
An antimetabolite: a drug that interfere with one or more enzymes or their reactions that are necessary for DNA synthesis. Originally used in cancer treatment because it destroys rapidly-dividing cells. As an abortifacient it destroys trophoblast cells: i.e. tissue that later becomes the placenta. |
DRUGS USED to INDUCE ABORTION
MIFEPRISTONE
(antiprogestogen progesterone-receptor blocker, causes death and detachment of
placenta)
A progesterone-blocker, when used to induce abortion the drug causes decidual necrosis (death of placental and chorionic tissue)*, leading to detachment of the placenta and death of the embryo/fetus
* "The effects of mifepristone on the structure of human decidua and chorion and Bax and Bcl-2 expression at early stage of pregnancy." Fei Tian, Hua Han, et.al. BMC Pharmacology and Toxicology vol. 23, Art.: 55 (July 23, 2022)https://bmcpharmacoltoxicol.biomedcentral.com/articles/10.1186/s40360-022-00592-4
Mifepristone is a steroidal antiprogestogen (IC50 = 0.025 nM for the PR), as well as an antiglucocorticoid (IC50 = 2.2 nM for the GR) and antiandrogen (IC50 = 10 nM for the AR) to a much lesser extent. It antagonizes cortisol action competitively at the receptor level.
In the presence of progesterone, mifepristone acts as a competitive progesterone receptor antagonist (in the absence of progesterone, mifepristone acts as a partial agonist).
MISOPROSTOL
(prostaglandin – induces uterine contractions)
Misoprostol, a prostaglandin analog, binds to myometrial cells to cause strong myometrial contractions leading to expulsion of embryonic/fetal tissue. This agent also causes cervical ripening with softening and dilation of the cervix.
METHOTREXATE
Antimetabolite - destroys placental and embryonic/fetal tissue)
An antimetabolite: a drug that interfere with one or more enzymes or their reactions that are necessary for DNA synthesis. Used in cancer treatment because it destroys rapidly-dividing cells. As an abortifacient it destroys trophoblast cells: i.e. tissue that later becomes the placenta. Since the cells of the embryo/fetus are also rapidly-dividing, it is hard to imagine that methotrexate does not directly kill embryonic/fetal cells, as well..
Destroys trophoblast ( https://pubmed.ncbi.nlm.nih.gov/22510625/ ) “Methotrexate: the pharmacology behind medical treatment for ectopic pregnancy” Catherine S Stika, Clin Obstet Gynecol,2012 Jun;55(2):433-9.
From the Mayo Clinic page on medical abortion
https://www.mayoclinic.org/tests-procedures/medical-abortion/about/pac-20394687
Medical abortion can be done using these medicines:
Oral mifepristone (Mifeprex) and oral misoprostol (Cytotec). This is the most common type of medical abortion. These medicines are usually taken within seven weeks of the first day of your last period.
Mifepristone (mif-uh-PRIS-tone) blocks the hormone progesterone, causing the lining of the uterus to thin and preventing the embryo from staying implanted and growing. Misoprostol (my-so-PROS-tol), a different kind of medicine, causes the uterus to contract and expel the embryo through the vagina.
You may take the mifepristone in your provider's office or clinic. Then you might take the misoprostol at home, hours or days later.
You'll need to visit your health care provider again about a week later to make sure the abortion is complete. This regimen is approved by the Food and Drug Administration (FDA).
Oral mifepristone and vaginal, buccal or sublingual misoprostol. With this type of medical abortion, you take a mifepristone tablet by mouth. The next step is to use a slowly dissolving misoprostol tablet placed in your vagina (vaginal route), in your mouth between your teeth and cheek (buccal route), or under your tongue (sublingual route).
The vaginal, buccal or sublingual approach lessens side effects and may be more effective. To be most effective, these medicines must be taken within nine weeks of the first day of your last period.
Methotrexate and vaginal misoprostol. Methotrexate is rarely used for elective, unintended pregnancies, although it's still used for pregnancies outside of the uterus (ectopic pregnancies). This type of medical abortion must be done within seven weeks of the first day of your last period. It can take up to a month for methotrexate to complete the abortion. You receive methotrexate as a shot or a pill you take by mouth. The misoprostol is later used at home.
Vaginal misoprostol alone. Vaginal misoprostol alone can be effective when used before nine weeks of gestation of the embryo. But vaginal misoprostol alone is less effective than other types of medical abortion.
there are many states that have very few abortion providers, meaning that abortion is not effectively available to people without means to travel. For example, in Mississippi 99% of parishes (counties) do not have an abortion provider. Other states in which more than 95% of counties do not have abortion providers include Nebraska, the Dakotas, Kansas, West Virginia, Wisconsin and Wyoming.
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2003